


Driver Project 14 - The PRIEST Study for Low and Middle-Income Countries
To ensure hospitals in low- and middle- income countries are not overwhelmed during the COVID-19 pandemic by developing a risk assessment tool for clinicians to quickly decide whether a patient needs emergency care or can be safely sent home.
Carl Marincowitz and colleagues at the University of Sheffield in the United Kingdom and the University of Cape Town in South Africa have developed a risk assessment tool to help emergency clinicians quickly decide whether a patient with suspected COVID-19 needs emergency care or can be safely treated at home to avoid overburdening hospitals particularly in low- and middle- income countries (LMICs). They have used existing data to which they have access on 50,000 patients with suspected COVID-19 infection who sought emergency care in the United Kingdom, South Africa, and Sudan to develop prediction models for specific COVID-19 related outcomes in all income settings. These prediction models have been used to develop risk stratification tools, which enable providers to identify the right level of care and services for distinct subgroups of patients. These have been developed with input from patient and clinical stakeholders. The team have tested the performance of their risk assessment tools for identifying high-risk patients with existing triage methods.
Driver Project 14
| Title | Journal | Date |
Type | Abstract |
|---|---|---|---|---|
| PLOS ONE | June 2023 | Publication | Uneven vaccination and less resilient health care systems mean hospitals in LMICs are at risk of being overwhelmed during periods of increased COVID-19 infection. Risk-scores proposed for rapid triage of need for admission from the emergency department (ED) have been developed in higher-income settings during initial waves of the pandemic. | |
| BMJ – Emergency Medicine Journal | Nov 2022 | Publication | Tools proposed to triage acuity in suspected COVID-19 in the ED have been derived and validated in higher-income settings during early waves of the pandemic. We estimated the accuracy of seven risk-stratification tools recommended to predict severe illness in the Western Cape, South Africa… |
| Title | Type | Description |
| Pandemic Respiratory Infection Emergency System Triage. UK, South Africa, Sudan | Metadata | Variables PRIEST data patients attending ED with suspected COVID19 |
| Title |
Description |
|
| Watch: ICODA webinar Series: Privacy Enhancing Technologies (PETs): The use of Trusted Research Environments in global health research | Dr Carl Marincowitz, Principal Investigator of the PRIEST study from Sheffield University, UK, will describe their experiences of using TREs in their research projects. | 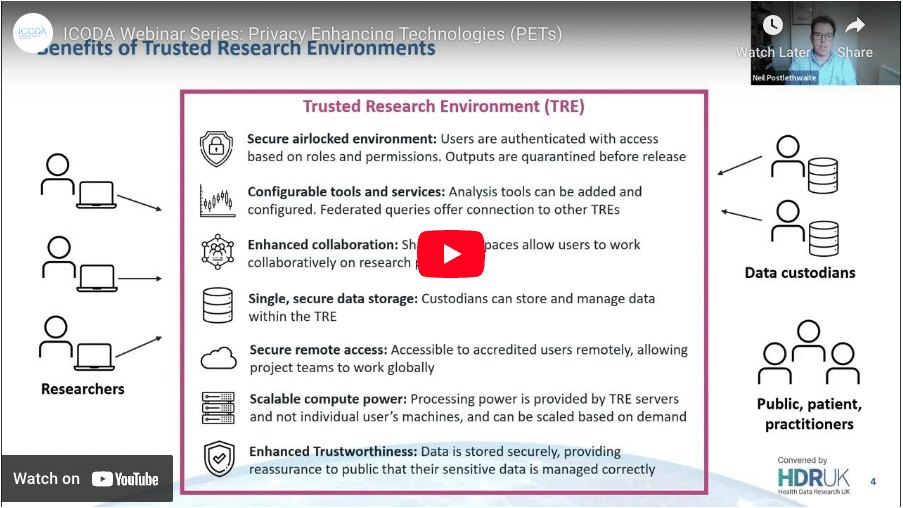
|
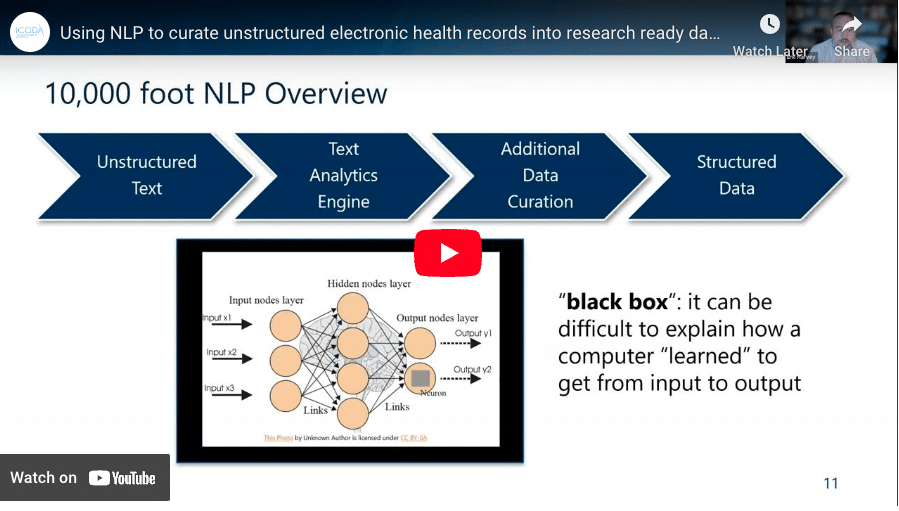
| Watch: ICODA Webinar Series: Using Natural Language Processing (NLP) to curate unstructured electronic health records into research ready datasets |
See NLP in action as part of the ICODA Grand Challenges ‘PRIEST’ project (Pandemic Respiratory Infection Emergency System Triage) Study for Low and Middle-Income Countries as a case study. |
|
Video Transcription
So what our project is aiming to do is to develop triage tools for serious adverse outcomes in an emergency care setting for patients with suspected COVID. So the background to this project is that in the UK during the first wave, we collected data from over 20,000 patients who attended emergency departments and across the UK, we’ve developed something called PRIEST score which can be used to predict death or requires organ support. And that’s being used to help determine whether when a patient comes to the emergency department and then need inpatient admission and that’s been adopted by things like the American College of Emergency Physicians. However, that’s only really applicable to high income settings as derived in the UK. So what we’re trying to do is derive similar tools which can be used to predict serious adverse outcomes in various settings. And in order to do that via collaboration with the university teacher, and so with Professor Lee Wallace’s team, and what they’ve got is routine data from the Western Cape. And also, they’ve worked but also called Dotty Jessimae, well in Sudan, and they also have a data set from two institutions into that. So we’re going to use the three datasets the UK datasets, the South Africans have nice data set to derive and validate tools which have a middle income setting, which repeats South Africa Western Cape and allow us all setup which is so we have three data sets. The first is the 20,000 patients from across the UK, attended the Magnus apartments in the fast way. The second data is routine, electronically captured data in the Western Cape of South Africa, which again was in the 10s of 1000s. And then the final data has been extracted from health care records in two sentences. So the main challenges so far appears on negotiation with different information governance landscapes and trees, which we’re working in with our collaborators, also curating and linking the reaching base with South Africa. is quite challenging, because it’s the best time to actually receive datasets for a project like this. But what’s really good is the secure Workbench is a place where we can share the data in a way that we can help deal with the information governance issues, and also the support. We’re getting from ICATER in terms of placement correction. I think developing contextually appropriate and accurate prediction tools for serious adverse outcomes for patients suspected COVID-19 in low and middle income countries, while also transparent and evidence based triage of need for inpatient admission and also sort of emergency healthcare resources more generally, in parts of the world where the vaccine rollout unfortunately, sort of lagging behind so highly concessive. We’re hoping that our first two sort of develops using the UK data sets and validates to the standards set around February or March in the DRC I believe so at least as a preprint sharer first finding spots, the analysis the Western Cape will vary a bit later. And then finally, we’ll hope to have every feature workshop by August.
1 So pulling and linking the large amounts of existing reaching data sets across the world and making them available to researchers in a way that complies with ethical and information governance requirements, but there’s also proportionate to what researchers are trying to do. And also making the data available in a way which researches to actually use a lot of the space very Byzantine and how it’s set up. And then sort of the second thing is building the metrological technical capacity to use these datasets, lots of important questions, especially in low and middle income countries, because there are very specific things about reaching datasets and how they’re different to datasets which should be flexible for the purposes of research.
I mean, the short answer is no. And the main thing is that because we are the University of Sheffield have a lot to teach now because of the work we’ve done in driving the original Prease score in terms of passenger space and develop the tools while the data that actually scandalise it from some lower middle income countries. So data sharing is facilitating us sharing our scale with our collaborators and help them with that analysis.
So I guess about a project very excited for us to do this, in a way which we can support collaboration with the University of Cape Town. There’s a lot of expertise which has been made available to support that collaboration which would otherwise and all the second facilities are generally.